Delivering Healthcare in America 7th Edition Chapter 11
Major Recommendations
- All health care settings should have a TB management or infection prevention and control program supported at the highest administrative level. This involves a hierarchical approach to infection prevention and control measures categorized as administrative, environmental and personal protection controls.
- Airborne precautions should be initiated immediately for everyone with suspected or confirmed respiratory TB disease admitted to a hospital. The criteria for discontinuation of airborne precautions include the following: establishment of an alternative diagnosis, clinical improvement, adherence to effective therapy, sputum smear and/or culture conversion, and drug-susceptibility tests that indicate fully sensitive organisms or low clinical suspicion of drug resistance.
- U.S. National Institute for Occupational Safety and Health ( NIOSH )-certified respirators (N95 or higher filter class) should be used by HCWs providing care for or transporting patients with suspected or confirmed respiratory TB disease.
- Masks should be used by patients/people with suspected or confirmed respiratory TB disease when outside an airborne infection isolation room.
- Baseline tuberculin skin testing (TST) is recommended for all HCWs in health care and community care settings. Recommendations for periodic and serial (repeated) TST for HCWs vary with the setting. Interferon-gamma release assays are not recommended for serial testing.
Introduction and General Principles
While the incidence of tuberculosis (TB) in Canada is generally low, exposure to people with unsuspected active respiratory TB disease followed by transmission of M. tuberculosis does occur in health care settings Footnote 1Footnote 2. A survey of TB control services in all Canadian provinces and territories in 2008 reported a total number of 1,562 cases of active TB disease and 11,935 people treated for latent TB infection (LTBI) Footnote 3. Approximately 50% of people with active TB disease in this survey were admitted to hospital for an average of 21 days. Although the overall number of people admitted to Canadian health care facilities with active TB disease is low, both health care and community settings (e.g. homeless shelters and drop-in centres) serving at-risk populations continue to pose a hazard for the transmission of M. tuberculosis Footnote 4Footnote 6. Populations at risk of active TB disease include people with a history of active TB disease; staff and residents of homeless shelters; urban poor; staff and inmates of correctional facilities, including previously incarcerated people; injection drug users; people born in Canada prior to 1966; Aboriginal Canadians; people infected with human immunodeficiency virus (HIV); those born or previously residing in countries with a high TB incidence (in Asia, Eastern Europe, Africa and Latin America); and HCWs serving these at-risk groups Footnote 7Footnote 10.
Literature reviews show that the incidence of LTBI among HCWs increases with certain occupational risk factors, including number of years working in health care settings where patients with active respiratory TB are cared for, providing direct care to those with respiratory TB disease, working in emergency departments or medical wards, providing services for patients infected with HIV, and participating in aerosol-generating medical procedures (e.g. sputum induction and bronchoscopy) on individuals with TB Footnote 5Footnote 11Footnote 12.
In hospitals, clinics, community care centres and correctional facilities, where people congregate and share indoor air (in the same room or via the building ventilation system), the risk of M. tuberculosis transmission can be increased if ventilation and other infection prevention and control measures are inadequate. In addition, exposure to people with active, undiagnosed and untreated respiratory TB disease has resulted in high rates of positive TST results in HCWs Footnote 1Footnote 2Footnote 5Footnote 13. Reported TB outbreaks within health care facilities are often due to failure to implement appropriate TB infection prevention and control measures Footnote 4. These observations have heightened concerns and resulted in the formulation of recommendations for the prevention of health care associated transmission of M. tuberculosis to HCWs, patients and visitors Footnote 7Footnote 14Footnote 15. A review of the literature suggests that implementation of a full hierarchy of infection prevention and control measures in many hospitals, as recommended in published guidelines, has led to successful reduction in M. tuberculosis transmission Footnote 5 and is therefore considered integral to preventing transmission in hospitals, other health care settings, and residential and community care facilities.
This chapter reviews factors that determine or affect transmission of M. tuberculosis within hospitals, other health care settings, and residential and community care settings while focusing on measures to prevent transmission. The term HCWs refers to individuals in health care settings who provide health care or support services, such as physicians, nurses, nurse practitioners, paramedics, emergency first responders, respiratory therapists, unregulated health care providers, clinical instructors, students, volunteers, and housekeeping, dietary and maintenance staff16.
Recommendations are based, as much as possible, on published evidence to date. However, the evidence applicable to infection prevention and control of M. tuberculosis that is based on randomized controlled trials, generally considered the strongest level of evidence, is limited. This type of study design is generally not feasible or practical when analyzing risk factors or situations involving natural exposure (e.g.TB outbreaks). As a result, the majority of the available evidence comes from observational studies, such as cohort or case-control studies, and from qualitative analyses of outbreaks. This chapter cites the evidence base from these primary studies, as well as from several published literature reviews Footnote 5Footnote 9Footnote 17 and from a systematic review that includes recommendations from the US Centers for Disease Control and Prevention (CDC) Footnote 7. Recommendations are itemized in boxes, tables or algorithms with the strength of the recommendation and the quality of its evidence indicated (refer to Preface for explanation of rating). Where detailed information is beyond the scope of this chapter or further references are of interest, refer to the relevant chapter(s) in this book.
Determinants of Transmission of Mycobacterium tuberculosis
Aerosolization of infectious M. tuberculosis bacteria occurs when individuals with respiratory TB disease cough, sneeze, sing, play wind instruments or speak. Cough-inducing procedures (e.g. bronchoscopy, sputum induction) as well as some laboratory and autopsy procedures can also cause aerosolization of mycobacteria. Once infectious M. tuberculosis bacteria are aerosolized, they are carried throughout a room or building by air currents and can be inhaled by another individual, with the possibility of resulting in TB infection. Although the risk of transmitting M. tuberculosis is highly variable, the presence of certain factors (refer to section Factors associated with increased risk of transmission of M. tuberculosis bellow) predicts an increased transmission risk. In general, the more of these factors present, the greater the risk of M. tuberculosis transmission. For further discussion on determinants of M. tuberculosis transmission, refer to Chapter 2, Transmission and Pathogenesis of Tuberculosis.
Factors Associated with Increased Risk of Transmission of M. tuberculosis
- Patient factors
- Respiratory (pulmonary or laryngeal) disease Footnote A
- Number of Patients with Respiratory TB Disease Footnote A
- Respiratory secretions that are acid-fast bacteria (AFB) smear positive
- Presence of cough
- HIV infection Footnote A
- Atypical manifestations of disease
- Diagnostic/laboratory risk factors
- Cough-inducing procedures, e.g. sputum induction, bronchoscopy or administration of aerosolized therapies
- Delayed diagnosis Footnote A
- Autopsy and preparation of pathology specimens
- Improper handling of laboratory specimens containing M. tuberculosis
- Treatment factors
- Incorrect, ineffective or no therapy Footnote A
- Delayed treatment
- Environmental factors
- Inadequate ventilation to remove airborne infectious M. tuberculosis Footnote A
- Inadequate TB infection prevention and control measures for containment of M. tuberculosis
- Duration of exposure and proximity to infectious patient Footnote A
- Overcrowding Footnote A
- Absence of sunlight
- High humidity
- Footnote A
- These factors are discussed below.
Respiratory (Pulmonary or Laryngeal) TB Disease
People with laryngeal TB disease show the highest infectivity of all forms of TB. While most people with nonrespiratory TB alone are not infectious, it is important to exclude concomitant respiratory involvement, which occurs in a significant proportion of those with nonrespiratory TB Footnote 18. Pleural TB disease in the absence of concomitant respiratory involvement is not considered infectious, refer to Chapter 2, Transmission and Pathogenesis of Tuberculosis.
Number of Patients with Respiratory TB Disease
It is generally understood that the number of hospitalized patients with respiratory TB disease, particularly before diagnosis and treatment, is an important determinant of institutional transmission risk. Results from one study involving 17 acute-care hospitals in Canada showed that with effective implementation of infection prevention and control measures the number of patients might not be the best indicator of transmission risk. In this study, institutional risk of M. tuberculosis transmission was found to be better correlated with delayed diagnosis and treatment Footnote 19 .Thus, prompt diagnosis followed by early isolation and appropriate treatment has a mitigating effect on this risk factor Footnote 5.
HIV Infection
There is no clear evidence that people infected with M. tuberculosis are more infectious if they are coinfected with HIV. However, there will often be rapid development of active TB disease, Footnote 20 and HIV-related TB disease will often have atypical clinical manifestations, leading to delayed diagnosis. The increased risk of M. tuberculosis transmission by this population is related to the potential for delayed isolation if the index of suspicion for respiratory TB disease is low. Also, refer to Chapter 10, Tuberculosis and Human Immunodeficiency Virus.
Delayed Diagnosis
Refer to section "Identification of patients with active respiratory TB within hospitals" in this chapter.
Incorrect, Ineffective or No Therapy
The administration of incorrect or ineffective therapy or no therapy at all contributes to the risk of transmission. Refer to Chapter 5, Treatment of Tuberculosis Disease.
Inadequate Ventilation
The exchange of indoor air with outdoor air reduces the risk of infection by diluting the concentration of viable airborne M. tuberculosis bacteria present Footnote 1. Theoretically, the risk of transmission should decrease exponentially with increasing fresh-air ventilation.
Duration of Exposure and Proximity to Infectious Patient
The risk of TB infection varies with duration of exposure, form of tuberculous disease and type of patient care activity. In one study, an hour of exposure during bronchoscopy on a patient with unrecognized smear-positive disease resulted in a 25% risk of infection Footnote 12 and in another study exposure to a patient with laryngeal TB resulted in a 1.7% risk of infection per hour Footnote 21. Even when the relative risk of infection is low, repeated exposure can lead to a higher cumulative risk. For example, if a HCW is exposed for 1 hour each week, the cumulative risk can approach 100% after 10 years of repeated exposure.
Overcrowding
Overcrowding contributes to transmission in settings like homeless shelters and correctional facilities. The relative importance of select factors (such as overcrowding, duration of exposure and proximity to infectious people in a confined space) to M. tuberculosis transmission has not been quantitatively described in the literature, but some reports suggests that their impact is highly variable Footnote 22.
Risk Classification
Health Care Settings
The risk of health care associated transmission of M. tuberculosis to HCWs, patients (or residents) and visitors varies with the type of setting, occupational group, effectiveness of TB infection prevention and control measures, and patient/resident population Footnote 7. A review of the community profile of TB disease, as well as the risk category of the health care facility and unit, can be used to conduct facility and/or unit risk assessments. This provides a framework for institutions to predict whether their workers are at increased risk of TB exposure so that the necessary infection prevention and control strategies can be implemented.
An approach to classifying risk of M. tuberculosis transmission in health care settings is described in Table 1. The risk categories presented have been modified from previous classifications Footnote 4Footnote 23 and are based upon review of the available literature Footnote 7. While the number of people with respiratory TB disease in a facility during a year is considered a key determinant of transmission risk, the likelihood of exposure to any one patient or resident can vary considerably among facilities. To account for this, the classification below is based on the number of active patient or resident beds and number of cases of respiratory TB disease diagnosed in the facility in a typical year.
| Risk category | Facility size | Number of active TB cases present annually |
|---|---|---|
| ||
| Low | Hospitals: ≥200 beds | <6 |
| Hospitals: <200 beds | <3 | |
| Long-term care institutions including homes for the aged, nursing homes, chronic care facilities, hospices, retirement homes, designated assisted living centres and any other collective living centre | <3 | |
| Not considered low | Hospitals: ≥200 beds | ≥6 |
| Hospitals: <200 beds | ≥3 | |
| Long-term care institutions (as listed above) | ≥3 | |
| Infirmaries in correctional facilities Table 1 - Footnote A | ≥3 | |
HCW Activities
Patient care activities performed by HCWs are associated with varying degrees of exposure risk and subsequent infection with M. tuberculosis (Refer to section Risk categories for activities performed by health care workers). This risk increases with the duration of exposure and higher amounts of airborne mycobacteria. As a result, it is recommended that HCWs perform a risk assessment prior to interactions with people suspected of or confirmed as having active TB disease Footnote 16. This risk assessment involves evaluating the likelihood of exposure to M. tuberculosis for a specific patient care activity, with a specific patient, in a specific environment and under particular conditions. This is referred to as a point-of-care risk assessment and is described in a recent publication from the Public Health Agency of Canada (PHAC) Footnote 16. The assessment informs HCWs' decisions regarding the appropriate infection prevention and control measures needed to minimize the risk of exposure for themselves, other HCWs, patients and visitors.
Risk Categories for Activities Performed by Health Care Workers
- High-risk activities
- Cough-inducing procedures (such as sputum induction)
- Autopsy
- Morbid anatomy and pathology examination
- Bronchoscopy
- Mycobacteriology laboratory procedures, especially handling cultures of M. tuberculosis
- Intermediate-risk activities
- Work requiring regular direct patient contact on units (such as emergency departments) where patients with respiratory TB disease may be present Footnote A
- Work in pediatric units where patients with TB may be admitted Footnote B
- Cleaning of rooms of patients with respiratory TB disease
- Low-risk activities
- Work requiring minimal patient contact (such as clerical, reception and administration)
- Work on units where patients with respiratory TB disease are unlikely to be present Footnote C
- Footnote A
- This includes work done by all HCWs in these units.
- Footnote B
- Pediatric patients with respiratory TB disease should be considered infectious until infectiousness is ruled out by radiography and negative acid-fast bacteria sputum smears in patient, parents or caregivers. Refer to section "Isolation considerations for pediatric patients" in this chapter and Chapter 9, Pediatric Tuberculosis.
- Footnote C
- Classification of such units as low risk may be inaccurate if the population they are serving has a high incidence of TB (e.g. patients born or previously residing in countries with a high TB incidence or other at-risk populations). Some of the longest delays in diagnosis may occur in such settings.
Laboratory Personnel Handling M. tuberculosis
There are risks associated with handling M. tuberculosis in the laboratory that are not typically present in health care settings. Compared with the general population, laboratory HCWs have been found to have a greater risk of acquiring LTBI Footnote 7. Although this risk stems mainly from aerosol formation during specimen or isolate manipulation, other mechanisms of transmission have been described in this setting. At the time of publication of these Standards, PHAC's Laboratory of Biosafety and Biosecurity was in the process of preparing a biosafety guideline, Mycobacterium tuberculosis Complex (MTBC ) Biosafety Directive. Refer to Appendix D for details on laboratory standards. Recommendations on safe laboratory procedures, training programs, infection control plans, respiratory protection, TST screening for personnel and safe transportation of samples are also available from other sources Footnote 7Footnote 24Footnote 25.
Prevention and Control of Transmission of M. Tuberculosis
Current recommendations for the prevention of health care associated transmission of M. tuberculosis involve a hierarchical approach to infection prevention and control measures, including the following:
- Administrative controls - institutional policies or measures that aim to reduce the time between the arrival of people with respiratory TB disease at a health care facility, diagnosis of their condition and placement in an airborne infection isolation room ( AIIR ). The purpose of these policies is to provide overarching protection for all HCWs, patients and visitors in a facility. Administrative control measures include occupational health programs incorporating skin testing of HCWs for LTBI after exposure and at regular intervals, access to treatment of LTBI, exclusion of HCWs with respiratory TB disease, facility and unit risk assessments, as well as a HCW education program. Details on performing a risk assessment and on HCW education can be found elsewhere Footnote 7Footnote 16.
- Environmental (engineering) controls - environmental measures to reduce the likelihood of exposure of HCWs, other patients and visitors to viable airborne M. tuberculosis. These include mechanical ventilation systems (to supply clean air) in patient care areas, use of ultraviolet germicidal irradiation (UVGI) and high-efficiency particulate air (HEPA) filters.
- Personal protection controls - measures directed to individual HCWs either to prevent infection (such as use of respirators) or to prevent disease if infected (such as detection and treatment of LTBI).
Each control measure is further explained below.
Administrative Controls within Hospitals
Recommendations
(Conditional recommendations, based on very weak evidence)
All hospitals, regardless of risk category, should have a TB Management Program (or TB Infection Prevention and Control Program) supported at the highest administrative level with components detailed below. This program may be facilitated through existing infection prevention and control programs with administrative responsibility clearly delineated.
Other health care settings may refer to the hospital TB Management Program to identify procedures that are applicable to the setting.
Tuberculosis Management Program
The goal of a TB management program is to prevent M. tuberculosis transmission to HCWs, patients and visitors.
Risk Assessment
The first step of an effective TB management program in a hospital or other health care setting should be to perform an organizational risk assessment in order to decrease the risk of patient and HCW exposure to and acquisition of M. tuberculosis. The exposure risk for HCWs engaged in different activities should be evaluated during this assessment. For further information on an organizational risk assessment, refer to a recent PHAC publication Footnote 16.
In hospitals of all risk categories, the following features should be in place as components of the TB management program:
- Policies and procedures should clearly delineate administrative responsibility for developing, implementing, reviewing and evaluating various program components. The evaluation should include quality control and audits for all components of administrative, environmental and personal protection controls. Personnel with responsibility for the program within the facility should be designated.
- Policies and procedures should be in place for rapid identification, isolation and treatment of patients; reduction of health care associated transmission through environmental controls; and protection of staff through appropriate use of personal protective equipment, education and TST.
- An annual review of the indices of health care associated transmission should be done. This includes (i)TST conversion rates among HCWs; (ii) the total number of people with respiratory TB disease admitted annually; (iii) the number of occupational exposure episodes (i.e. admitted individuals with respiratory TB disease who were not placed under airborne precautions while receiving care); and (iv) the number of previously admitted patients whose TB was diagnosed only at autopsy.
- An annual summary of the clinical, epidemiologic and microbiologic features of patients whose TB is diagnosed within the hospital should be made available to HCWs caring for these patients. This will increase awareness of which patients in the population served are at risk of respiratory TB disease and the clinical manifestations.
- Additional considerations (such as higher index of suspicion or increased vigilance to prevent transmission before diagnosis) are recommended when caring for immunocompromised patients, whose infection may carry a higher risk of progression from LTBI to active TB disease. This includes patients in oncology, HIV and haemodialysis units or clinics.
In hospitals that are not considered low risk (Table 1), the following additional items should be in place as components of the TB Management Program:
- The hospital Infection Prevention and Control Committee (or other appropriate existing committee) should be given responsibility for the TB management program. Committee members should include people with day-to-day responsibility for infection prevention and control. There should also be representation from senior administration; occupational health and safety; laboratory, nursing and medicine; and other health disciplines or groups as needed (e.g. respiratory technology, public health, central supply, housekeeping, laundry, pharmacy, physical plant and maintenance).
In low-risk hospitals (Table 1), the following additional items should be in place as components of the TB management program:
- The TB management program may consist of screening protocols for diagnosis in patients with symptoms of respiratory TB disease and pre-arrangement to transfer all such patients to another centre where appropriate environmental measures are available.
- In hospitals with a transfer-out policy, there should be at least one separate, well-ventilated area Footnote 26 or a single room with the door closed, away from high-risk patients, Footnote 16 where patients can be maintained until they are transferred.
- Hospital administrators in collaboration with appropriate jurisdictional authorities, should coordinate the planning of adequate numbers of hospitals with resources to receive such patients with minimum delay.
Education of HCWs
A very important component of any TB management program is education of HCWs on how to protect themselves from exposure to M. tuberculosis. HCWs should be educated about TB infection prevention and control measures at the time of hiring and periodically thereafter. Education for HCWs should be relevant to their duties. For health care professionals, this should include awareness of epidemiologic and medical risk factors for TB, signs and symptoms of active TB disease (respiratory and nonrespiratory) and mechanisms of transmission. All HCWs, including orderlies, housekeeping and maintenance staff, should be educated to respect signage and to understand the importance of administrative, environmental and personal protection controls in the prevention of transmission.
Identification of Patients with Respiratory TB Disease Within Hospitals
Delayed diagnosis occurs in almost half of all hospitalized patients in whom respiratory TB disease is subsequently detected. This often results in significant exposure for HCWs and other patients. One study found that for each unrecognized case of respiratory TB disease, an average of 24HCWs were exposed Footnote 27. Certain locations within the hospital, such as emergency departments, are a frequent point of first contact with the health care system for people with undiagnosed respiratory TB disease Footnote 28Footnote 29. This was observed in a Canadian study: from 1994 to 1998, 47% of 250 people with TB made a total of 258 visits to emergency departments during the 6 months before their diagnosis Footnote 28.
Recommendations
(Conditional recommendations, based on strong evidence)
- A cough of 2- 3 weeks' duration with or without weight loss and fever in a person belonging to one of the at-risk groups below should prompt a thorough investigation to determine whether active respiratory TB is the cause: Footnote 7Footnote 10
- People with a history of active TB;
- Staff and residents of homeless shelters;
- The urban poor;
- Staff and inmates of correctional facilities and previously incarcerated people;
- Injection drug users;
- Aboriginal Canadians residing in communities with high TB rates;
- People infected with HIV;
- People born in Canada and other low TB incidence countries prior to 1966;
- People born or previously residing in countries with a high TB incidence in Asia, Eastern Europe, Africa and Latin America;
- People with high risk factors listed in Chapter 6, Table 1;
- HCWs serving at-risk groups.
To consider someone a suspect for active respiratory TB disease (for investigation and/or initiation of airborne precautions), cough of 2 weeks duration is a more sensitive criterion, but cough of 3 weeks duration will be more specific. Selection of 2 or 3 weeks as the criterion depends on the local experience and epidemiology of TB.
The TB incidence rate in Canada prior to 1966 was similar to that in a high TB incidence country (refer to Chapter 1, Epidemiology of Tuberculosis in Canada) thus the inclusion of this birth cohort as an at-risk group.
Concomitant respiratory TB disease should be ruled out in cases of nonrespiratory TB. Refer to Chapter 2, Transmission and Pathogenesis of Tuberculosis, and Chapter 7, Nonrespiratory Tuberculosis.
Prompt diagnosis of active respiratory TB can be a major challenge if the clinical features of TB are atypical, such as negative AFB sputum smears, non-cavitary lesions on chest radiograph and the absence of cough and sputum production Footnote 19. Atypical features of respiratory TB disease are more frequently observed in the elderly and people who are immunocompromised because of medical conditions (renal failure, HIV) or therapy (steroids, anti-tumour necrosis factor). Refer to Chapter 3, Diagnosis of Active Tuberculosis and Drug Resistance.
Airborne Precautions for Patients with Suspected or Confirmed Respiratory TB Disease
Recommendations
(Strong recommendations, based on strong evidence)
- Airborne precautions should be initiated as soon as possible for all those with suspected or confirmed respiratory TB disease who are admitted to a hospital.
- Patients (including children of any age) who show signs and symptoms of TB, or whose respiratory secretions, e.g. sputum or bronchial alveolar lavage, have yielded AFB, or who have a chest radiograph indicative of active TB should be immediately isolated in an AIIR. Refer to Figure 1.
Recommendations
(Conditional recommendations, based on very weak evidence)
- Once airborne precautions have been initiated, the patient should remain in the AIIR until isolation is discontinued by designated medical personnel. Patients kept under airborne precautions can leave an AIIR for medical reasons.
- A patient may be allowed to leave an AIIR but only if it can be ensured that he or she adheres to airborne precautions; these include the proper wearing of a mask.
- Refer to Figure 1 for detailed recommendations.
In the absence of an AIIR, the patient should be placed into a single room (with the door closed and a portable air filtration unit used if available) until transfer to a facility where an AIIR is available. Airborne precautions also include the use of respirators by HCWs caring for patients with suspected or confirmed active TB disease.
Isolation Considerations for Pediatric Patients
If isolation in the hospital is necessary for young children (under 5) with suspected or confirmed respiratory TB disease, it should be noted that they likely acquired their disease from adult family contacts, who may pose a risk to HCWs and other patients while visiting. Thus, for these patients, considerations for infection prevention and control in the hospital should include potentially infectious family members Footnote 30Footnote 31. Visitors (limited to immediate adult family or guardians) should be screened by symptoms and radiography for active TB disease and should wear a mask during visits (when not in the AIIR) until active TB disease is ruled out. Refer to Chapter 9, Pediatric Tuberculosis, for information on TB infection and disease in children.
Figure 1. Recommended steps for isolation for suspected or confirmed active respiratory TB disease in hospitalA
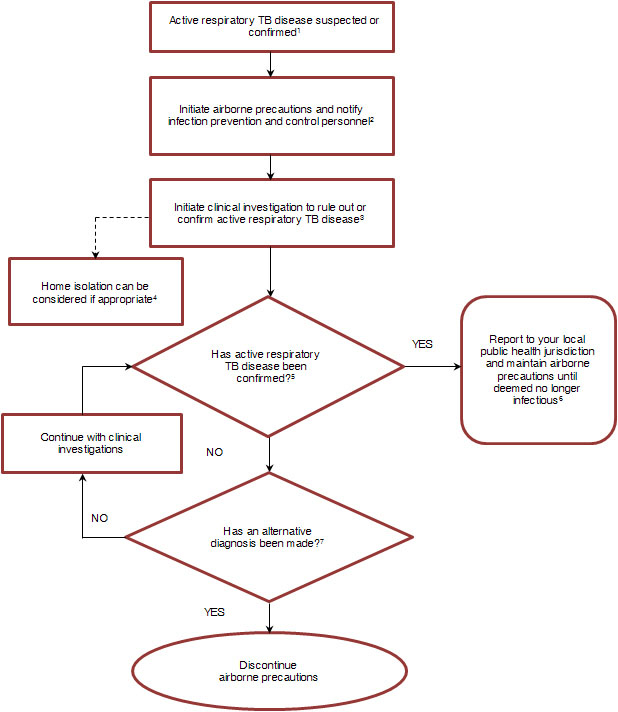
Figure 1. Legend
A) Includes infirmaries in correctional facilities
1) It is recommended that patients suspected of having active respiratory TB disease be isolated immediately rather than wait for confirmation of disease prior to initiating airborne precautions.
Airborne precautions are recommended during procedures that may generate aerosols from wound drainage in non-respiratory active TB disease.
Refer to Chapter 3, Diagnosis of Active Tuberculosis and Drug Resistance.
2) Airborne precautions include (in addition to routine practices):
- placement in an AIIR;
- respirator use by healthcare workers and if deemed necessary, by visitors also;
- mask use by patient when out of AIIR;
- restriction of patient to AIIR except for medically essential procedures;
- education of patient, families and visitors on the precautions.
Visitors should be restricted to immediate family or guardians. Visiting family or guardians of pediatric patients should be screened for active respiratory TB disease. Visits by children under age five and immunocompromised persons should be discouraged.
3) Cough inducing procedures (e.g., sputum specimen collection, sputum induction) should be performed in an AIIR.
Refer to Chapter 3, Diagnosis of Active Tuberculosis and Drug Resistance, for details of clinical investigations.
4) Refer to Figure 2 Legend for conditions for home isolation.
5) The examination of smears of respiratory specimens for acid-fast bacteria is widely used as a presumptive rapid test, however mycobacterial culture provides a definitive diagnosis of active TB disease.
6) Airborne precautions may be discontinued when the patient has clinical evidence of improvement, three consecutive negative sputum smears for acid-fast bacteria and there is evidence of adherence to at least two weeks of effective therapy. Multi-drug resistant TB cases and those with mono-resistance to rifampin (RMP) should have three consecutive negative sputum cultures after six weeks of incubation prior to discontinuing airborne precautions.
7) Airborne precautions can be discontinued if another diagnosis is made (e.g., cancer, non-tuberculous pneumonia) and concomitant active respiratory TB disease is considered unlikely.
AIIR: airborne infection isolation room
Transport of Patients with Suspected or Confirmed Respiratory TB Disease
Recommendations
(Conditional recommendations, based on very weak evidence)
- Prior to transport, HCWs involved in patient transport, transport personnel and the receiving health care facility should be advised of the infectious state of the patient.
- Patients should be escorted by a HCW during transport/transfer of patients from one facility to another or within a facility.
- Patients with respiratory TB disease should wear a mask, and HCWs involved in transport should wear a respirator (Refer to section "Respirators and masks").
- If transport between facilities is required, patients should not use public transport.
- Patients should be transported in well-ventilated vehicles (i.e. with the windows open when possible).
- Where air transport is required (e.g. from remote settings), transport personnel should refer to their organization's policies on medical transport of patients with airborne infections.
Preventing Patient-to-Patient Transmission of M. tuberculosis Within Hospitals
Measures should be taken to reduce the risk of M. tuberculosis transmission to people within the hospital, including patients, HCWs, other staff, volunteers and visitors. Until placement in an AIIR, a patient with suspected or confirmed active respiratory TB should wear a mask as a source control measure to prevent viable M. tuberculosis from being disseminated (refer to section "Respirators and masks"). Source control measures, patient placement in a single room and limiting of patient movement all contribute to reducing the risk of patient-to-patient transmission Footnote 16. When availability of single rooms is limited, priorities for placement of patients should be determined by risk assessment. Patients with suspected or confirmed respiratory TB disease have priority and should not share rooms with each other, since their strains and levels of infectivity may be different Footnote 16.
A review of HCWs' LTBI screening records for conversions as well as patient surveillance data and medical records for cases of respiratory TB disease can help to identify whether patient-to-patient transmission occurred before initiation of airborne precautions. This possibility should be considered under the following circumstances: Footnote 7
- A high proportion of people with respiratory TB disease were admitted to or examined in the same setting during the year preceding onset of their disease.
- Isolates from multiple patients in the same health care facility have identical anti-mycobacterial susceptibility and molecular genotypes.
- An increase occurred in the number of people with drug-resistant respiratory TB disease compared with the previous year (applicable if the transmission was from a drug-resistant patient).
Refer to Chapter 12, Contact Follow-up and Outbreak Management in Tuberculosis Control, for further information.
Discontinuation of Airborne Precautions
Institutional policies should designate people with the authority (e.g. the infection prevention and control personnel) to discontinue airborne precautions as well as manage both breaches of and adherence to airborne precautions.
Recommendations
(Strong recommendations, based on moderate evidence)
Suspect TB cases
- Airborne precautions may be discontinued if three successive samples of sputum (spontaneous or induced) are negative on smear unless TB is still strongly suspected and no other diagnosis has been made Footnote 24Footnote 32Footnote 33.
Note: Where feasible, three sputum specimens (either spontaneous or induced) can be collected on the same day, a minimum of 1 hour apart with at least one of them taken in the early morning. As previously done, the evidence used to inform sputum collection recommendations for discontinuation of airborne precautions originates from available studies related to diagnosis of respiratory TB disease. Refer Chapter 3, Diagnosis of Active Tuberculosis and Drug Resistance for the current evidence base.
A single negative AFB smear from bronchial alveolar lavage does NOT definitively exclude respiratory TB disease; three induced sputa provide superior yield for the diagnosis and therefore are preferred to a single bronchoscopy. Refer Chapter 3, Diagnosis of Active Tuberculosis and Drug Resistance, for further explanation and references.
Confirmed TB cases
Although the degree and duration of infectiousness of patients after initiation of effective therapy remains unclear, it is known that effective therapy (i.e. therapy with two or more drugs to which the TB organisms are susceptible) will rapidly reduce cough and the number of viable bacteria in the sputum.
Note: Drug susceptibility test results are usually available within 4 weeks in a smear-negative, culture-positive case and 3 weeks in a smear-positive case; this confirms the effectiveness of therapy to date. Refer to Appendix D on Tuberculosis and Mycobacteriology Laboratory Standards: Services and Policies.
Recommendations
(Strong recommendations, based on moderate evidence)
Confirmed TB cases
- Patients with smear-negative, culture-positive drug-susceptible respiratory TB:
These patients should be kept under airborne precautions until there is clinical evidence of improvement and a minimum of 2 weeks of effective therapy has been completed. Patients may be discharged to home isolation for the period requiring airborne precautions provided there is clinical improvement, drug-resistant TB is not suspected and there is no contraindication for home isolation (refer to Figure 2).
- Patients with smear-positive, culture-positive drug-susceptible respiratory TB:
These patients should be kept under airborne precautions until there is clinical evidence of improvement, evidence of adherence to at least 2 weeks of effective multidrug therapy based on the known antibiotic sensitivity of the patient's organism, and three consecutive negative AFB sputum smears Footnote 34. Patients may be discharged to home isolation for the period requiring airborne precautions provided there is clinical improvement, drug-resistant TB is not suspected and there is no contraindication for home isolation (Figure 2).
Note: Specimens can be collected within 1 hour of each other on the same day, with at least one of them taken in the early morning. As previously done, the evidence used to inform sputum collection recommendations for discontinuation of airborne precautions originates from available studies related to diagnosis of respiratory TB disease. Refer to Chapter 3, Diagnosis of Active Tuberculosis and Drug Resistance for the current evidence base. In patients who are no longer able to spontaneously produce a sputum specimen, sputum induction is useful and appropriate. More invasive testing, such as bronchoscopy, is not recommended for monitoring response to therapy.
Although smear-positive patients are still potentially infectious, their household contacts have already been heavily exposed and are often receiving therapy for LTBI when discharge from hospital is being considered. Thus, the risk of further transmission to these contacts should be balanced by the social, mental and physical health benefits of the patient's return home.
Recommendations
(Strong recommendations, based on moderate evidence)
Confirmed TB cases
- Patients with persistent smear-positive sputa: Patients may be discharged to home isolation for the period requiring airborne precautions provided there is clinical improvement, drug-resistant TB is not suspected and there is no contraindication for home isolation (Figure 2). If sputum specimens continue to be culture-positive after 4 months of anti-tuberculosis treatment or if culture results become positive after a period of negative results, drug susceptibility tests should be repeated and a TB expert consulted Footnote 7.
- Patients known to have active multidrug-resistant TB or mono-resistance to RMP : These patients should be kept under airborne precautions for the duration of their hospital stay or until three consecutive sputum cultures (not smears) are negative after 6 weeks of incubation. Also refer to Chapter 8, Drug-resistant Tuberculosis.
Figure 2. Recommended steps for isolation for suspected or confirmed active respiratory TB disease in the home
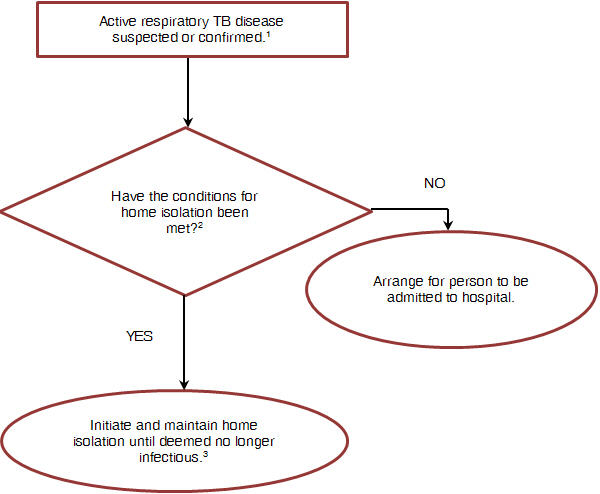
Figure 2. Legend
- Supervised therapy, if indicated, has been arranged;
- The person does not share a common airspace with non-household members (e.g., rooming house) and the household air is not being recirculated to other housing units (e.g., apartment complex);
- All household members have been previously exposed to the person. If any household members are TST negative, they should be informed and understand the potential risks;
- No children under the age of 5 or persons with immunocompromising conditions are present in the home (an exception would be if they are receiving prophylaxis or treatment for active TB disease or latent TB infection);
- No visitors should be allowed in the home except for HCWs;
- The person is counselled on and is willing and able to comply with limitations to their movement outside of the home (e.g., does not go to work, school or any other public indoor environment);
- The person should not be allowed to use any form of public transportation (if absolutely necessary, a taxi can be used to attend essential healthcare appointments provided the person is wearing a mask);
- The person should be allowed to ambulate outdoors since the risk of transmission is negligible provided they are not in very close contact with susceptible individuals for prolonged periods of time.
3) Home isolation may be discontinued when the patient has clinical evidence of improvement, three consecutive negative sputum smears for acid-fast bacteria and there is evidence of adherence to at least 2 weeks of effective therapy. Multi-drug resistant TB cases and those with mono-resistance to RMP should have three consecutive negative sputum cultures after 6 weeks of incubation prior to discontinuing home isolation. HCWs: health care workers.
Environmental (Engineering) Controls Within Hospitals
Ventilation Guidelines
Ventilation recommendations for AIIRs and select areas in hospitals are of critical importance because of their impact on reducing the risk for health care associated transmission of M. tuberculosis. Increasing air changes per hour (ACH) from 1ACH to 6ACH will result in four to five times more rapid clearing of infectious microorganisms from the air within a room. However, further increases above 6ACH will have progressively less effect, and increases above 12ACH may provide minimal additional benefit Footnote 29Footnote 35. In general, as air exchange rates are increased, there are increased costs for building and maintaining the ventilation system.
A number of recognized organizations have made recommendations regarding ventilation levels to reduce the risk of health care associated transmission of airborne pathogens, including M. tuberculosis and varicella-zoster viruses Footnote 7Footnote 36Footnote 37. These organizations have published different ventilation standards for AIIRs and other patient care areas within hospitals (refer to Table 2). Differences among these recommendations are not based on consideration of different evidence but, rather, on the risk-benefit assessment of each organization. Refer to Table 2 for current ventilation recommendations by different organizations.
General hospital areas
It is important to ensure that there is adequate ventilation in general (i.e. non-isolation) areas such as inpatient rooms and examination or treatment rooms. This is because people with unsuspected respiratory TB disease may be placed in them, posing a risk of transmission to other patients and HCWs Footnote 1. Recent literature on room ventilation rates has not provided definitive evidence for the ideal number of ACH to prevent transmission of TB in non-isolation rooms within hospitals Footnote 38.
Airborne infection isolation rooms (all hospitals except low risk with transfer-out policy)
Measures to ensure that adequate ventilation is in place are outlined below and are also discussed in more detail in other guidelines Footnote 7Footnote 16.
Recommendations
(Strong recommendations, based on moderate evidence)
- With the exception of rooms in which operative procedures are done, the direction of air flow should be inward from the hall into the room (negative pressure), and then the air should be exhausted outdoors. If an anteroom is used, the air from both the anteroom and patient room should be exhausted outdoors Footnote 16. To achieve this, the ventilation system should be designed to function such that the anteroom and/or the AIIR are at lower pressure relative to the hallway outside. An anteroom is not essential if the pressure differential is adequate. Refer to the CDC 's recent recommendations on pressure differentials Footnote 7.
- Windows and doors should be kept closed at all times, including during and after aerosol-generating procedures (long enough for air clearance in the room). Opening the window may cause reversal of the direction of air flow, depending upon the prevailing wind direction and outdoor temperature.
- Air should be exhausted to the outdoors through a dedicated exhaust system, ideally exiting from the roof of the building. It is important that the exhausted air does not re-enter the building or an adjacent occupied building. If the air will be recirculated, or if the exhausted air could re-enter the building, it should be passed through a HEPA filter before being exhausted Footnote 7. Within existing facilities, use of HEPA filtration units that recirculate air back into the room and/or ultraviolet germicidal irradiation (which has bactericidal activity against M. tuberculosis) may be adjunctive methods to remove or reduce viable airborne M. tuberculosis; these are discussed later in this chapter.
- The rate of air changes and direction of air flow should be verified at least every 6 months when the room is not being used as an AIIR. When the AIIR is in use, the direction of air flow should be verified daily using electronic pressure monitors, and should be recorded. Where electronic monitors are unavailable, such as in older buildings, in resource-constrained settings or in temporary isolation settings, smoke tubes placed at all four corners of the door can be used Footnote 16.
- The number of AIIRs required in hospitals not considered low risk should be based on the number of patients admitted each year with suspected respiratory TB disease. In organizations with very few admissions for TB, the number of AIIRs should be decided by the organizational authorities according to an analysis of AIIR utilization in the previous 2 or 3 years. The Canadian Thoracic Society suggests one or two more AIIRs than what was needed in the past at peak times. Appropriate resources should be made available to hospitals that will have such rooms and therefore receive patients with respiratory TB disease.
Sputum induction and administration of aerosolized pentamidine (all hospitals)
Recommendations
(Strong recommendations, based on moderate evidence)
- The smaller the room where these procedures are performed the easier and more practical it is to achieve required ventilation levels. Ideally, specially constructed "booths" (which are commercially available) should be used.
- Doors and windows should remain closed during and after the procedure, long enough for air clearance in the room (refer to Table 3).
- The air should be exhausted through a dedicated exhaust system or HEPA filtered.
Bronchoscopy and autopsy (all hospitals)
Areas where these procedures are performed tend to be much larger, making it difficult to achieve consistently high levels of ventilation with an inward direction of air flow. The increased risk of transmission associated with these activities warrants the significant expenditures required to achieve higher ventilation requirements.
Recommendations
(Strong recommendations, based on moderate evidence)
- Doors and windows should remain closed during and after the procedure, long enough for air clearance in the room (refer to Table 3).
- The air should be exhausted through a dedicated exhaust system or HEPA filtered.
| Area | Number of mechanical air changes per hour Recommending agency | Direction of air movement (all agencies) Table 2 - Footnote A | |||
|---|---|---|---|---|---|
| CTS (2013) | CSA (2010) | CDC (2005) | ASHRAE (2008) in FGI (2010) | ||
| |||||
| Autopsy suite | 12 | 20 | 12 | 12 | Inward |
| Bronchoscopy room | 6-12 Table 2 - Footnote B | 20 | 12 | 12 | Inward |
| Sputum induction/pentamidine aerosol | |||||
| Emergency department (waiting rooms) | 2 Table 2 - Footnote C | 12 15 | 12-15 | 12 | Inward |
| Trauma | 15 | ||||
| Radiology waiting rooms | 2 Table 2 - Footnote C | 9 | 12-15 | 12 | Inward |
| Operating room or surgical room | 15 | 20 | 15 | 20 | Outward |
| Airborne infection isolation rooms Table 2 - Footnote D | |||||
| Existing buildings | 6 | Table 2 - Footnote E | 6 | Table 2 - Footnote F | Inward |
| New buildings | 9 | 12 | 12 | 12 | |
| General patient care/non-isolation rooms | 2 Table 2 - Footnote C | 6 | Table 2 - Footnote G | 4 Table 2 - Footnote H | N/A |
Note that the CTS ventilation recommendations in Table 2 should be considered a minimum, as the CSA recommends higher ventilation rates for all areas. The CTS recommendations were developed on the basis of a systematic review of currently available published evidence. Specific ACH rates are not recommended here; rather, Table 2 provides health care organizations with current recommendations provided by various organizations. In deciding which recommendations to implement, hospital administrators may need to take into account factors such as resources, facility design and available scientific evidence. The current paucity of evidence for adequate ACH rates to prevent transmission of M. tuberculosis and gaps in existing literature indicate that further research is needed in this area.
Entering rooms after generation of infectious aerosols has ended or patient with respiratory TB disease has been discharged
Health care workers often ask when it is safe to enter a room previously occupied by a patient with respiratory TB disease without needing to wear a respirator or when a procedure room can be used for another patient after generation of infectious aerosols has ceased. As shown in Table 3, this is dependent upon the level of ventilation in the room (expressed as ACH), if room sizes are relatively similar.
| Air changes per hour | Minutes required for removal of airborne microorganisms | |
|---|---|---|
| 99% removal | 99.9% removal | |
| ||
| 2 | 138 | 207 |
| 4 | 69 | 104 |
| 6 | 46 | 69 |
| 12 | 23 | 35 |
| 15 | 18 | 28 |
| 20 | 14 | 21 |
| 50 | 6 | 8 |
The values apply to a room in which the generation of aerosols has ceased, and ongoing mixing of the air in the room is assumed. Consideration should also be given to keeping the relative humidity of the air in the hospital at ≤60%. This range has been cited to minimize environmental contamination and provide acceptable indoor air quality Footnote 7.
Cleaning of rooms
If a room previously occupied by a patient with respiratory TB disease has been ventilated for the appropriate amount of time (refer to Table 3), the routine hospital cleaning procedures used in non-isolation rooms may be used for terminal cleaning of AIIRs Footnote 7Footnote 16. If a room is still in use during cleaning, housekeeping personnel should wear a respirator (refer to section "Respirators and masks" below).
Ultraviolet Germicidal Irradiation
There is good evidence that short wave ultraviolet germicidal irradiation (UVGI) has excellent bactericidal activity against M. tuberculosis and can reduce infectious droplet concentrations by an amount equivalent to ventilation with 20 ACH, depending upon the room volume and type of lights used Footnote 39. Upper-room UVGI is considered a supplement or adjunct to ventilation Footnote 40. Use of UVGI has been controversial because of potential skin cancer and eye damage. However, the risk of skin cancer with new, commercially available UVGI units is essentially eliminated. Possible eye complications can be avoided by proper installation of these units above head height, as well as a schedule of regular inspection and maintenance. A detailed review of the use of UVGI was published in 2010 Footnote 41. This technology is being used with increasing frequency in settings such as homeless shelters to reduce airborne infectious microorganisms without the cost of renovating the heating, ventilation and air conditioning (HVAC) system. For further information on the safe and effective use of UVGI, including proper installation above head height and maintenance, refer to the recent CDC guidance document for using upper-room UVGI to control spread of M. tuberculosis in health care settings Footnote 40. Use of UVGI may be considered in bronchoscopy and sputum induction rooms, emergency departments, autopsy areas and HIV clinics if ventilation is inadequate and cannot be upgraded. It can also be used where exposure is unpredictable, such as emergency departments in hospitals that are not considered low risk (refer to Table 1).
High-efficiency Particulate Air (HEPA) Filtration
HEPA filtration can be used to filter the exhaust from airborne infection isolation rooms, bronchoscopy suites or rooms where sputum induction is performed. Small HEPA units, either fixed or portable, may also be used to filter recirculated air in a room without the need for an increase in the amount of outdoor air supplied. HEPA filters require careful monitoring and regular change, as clogged filters will result in decreased efficacy. People performing maintenance and replacing filters on any ventilation system that is probably contaminated with M. tuberculosis should wear a respirator Footnote 7 (refer to section "Respirators and masks"). For further information on HEPA filtration and details on safety issues when handling spent filters, refer to the CDC guidelines Footnote 7.
With both UVGI and HEPA filtration environmental controls, regular maintenance (including procedures for installation, removal and disposal) and corresponding documentation are necessary.
Personal Protection Controls Within Hospitals
Personal protection controls are the final level in the hierarchy of control measures for preventing health care associated transmission of M. tuberculosis.
Respiratory Protection Program
Respiratory protection is one element of personal protection control measures. All hospitals should have a respiratory protection program in place. An essential component of the program involves selecting appropriate NIOSH-certified respirators for HCWs, as discussed below. For cost-efficiency purposes, it is also important to provide respirator models with inherently good fit characteristics, as these have been shown to fit more than 90% of workers Footnote 42Footnote 43. The health care organization should ensure that appropriate respirators are available as needed for use by HCWs, other staff and visitors, contractors, etc., and that masks, as needed for use by patients with respiratory TB disease, are available.
Another essential component of a hospital respiratory protection program is education of HCWs regarding the occupational risk of TB and the role of respiratory protection in reducing that risk.
Respirators and Masks
Respiratory protection of HCWs involves the use of a respirator with a filter class equivalent to or higher than an N95, to prevent inhalation of aerosols containing infectious microorganisms. The most widely used respirators by HCWs in North America are the NIOSH-certified half-facepiece disposable respirators with an N95 filter class, commonly referred to as N95 respirators Footnote 15Footnote 16. These respirators are certified to filter 95% of particles of diameter 0.3 microns (µm) or larger with less than a 10% leak, thus protecting wearers against airborne infectious microorganisms such as M. tuberculosis. Footnote 7Footnote 44
A mask (either surgical or procedure) is used as a physical barrier. Masks are worn by HCWs to protect their skin and mucous membranes (nose and mouth) from droplets from an infected patient (or source). Masks are not designed for respiratory protection of HCWs as they are less than 50% effective in filtering small droplet nuclei (1-5 microns) containing M. tuberculosis Footnote 45.
Masks worn by patients with respiratory disease serve as a source control measure to trap the droplets that these patients expel. There is concern that because masks are loose-fitting they may allow the escape of airborne droplets (particularly during coughing); tight-fitting respirators, on the other hand, may be uncomfortable for patients (particularly those with limited respiratory reserve).
It is recommended that in all hospitals, including those with a transfer-out policy for cases of active TB disease, N95 respirators should be available for HCWs whenever a patient is suspected of or confirmed to have respiratory TB disease. This is particularly important because most low-risk hospitals will not have AIIRs in which to house patients while awaiting transfer.
Fit Testing
Fit testing is used to determine whether a particular size and model of respirator fits a given person by assessing leakage around the face-respirator seal. Each time HCWs put on a respirator, a user seal check (according to manufacturer's instructions) is required to determine whether the respirator is properly sealed to the face. When TB patients are housed in AIIRs, the contribution of respirators in preventing TB transmission to HCWs appears to be minimal Footnote 46. Hence, despite published literature on fit testing Footnote 47Footnote 49 there is insufficient evidence showing that a fit testing program results in reduced risk of health care associated transmission of M. tuberculosis. Nevertheless, most Canadian jurisdictions require fit testing for HCWs to determine their ability to obtain a satisfactory seal during respirator use Footnote 50. HCWs are referred to jurisdictional requirements regarding the processes and frequency of fit testing. In the absence of requirements, consult provincial/territorial public health authorities.
Respirator recommendations for HCWs
(Strong recommendations, based on strong evidence)
- NIOSH -certified respirators (N95 or higher filter class) should be used by HCWs providing care to patients with suspected or confirmed respiratory TB disease.
- NIOSH -certified respirators (N95 or higher filter class) should be used by HCWs involved in the transport of patients suspected of or confirmed as having respiratory TB disease, e.g. paramedics.
- Refer to jurisdictional requirements for fit testing of respirators.
Mask recommendations for patients
(Strong recommendations, based on strong evidence)
- Masks should be used by patients with suspected or confirmed respiratory TB disease when leaving their AIIRs.
- Masks should be used by patients with suspected or confirmed respiratory TB disease during transfer to a different location.
Screening for LTBI as Part of Infection Prevention and Control in Hospitals
Baseline TST (all HCWs in all health care facilities)
The importance of conducting proper baseline TST for all potentially exposed HCWs in all health care settings cannot be overemphasized. At the time of employment, many HCWs may already be TST positive because of prior exposure, particularly HCWs born or previously residing in countries with high TB incidence who may have been exposed and infected before moving to Canada. In addition, older Canadian-born HCWs in some provinces/territories may have received bacille Calmette-Guérin (BCG) vaccination, which can interfere with TST results. Prior exposure to M. tuberculosis, nontuberculous mycobacterial infection or BCG vaccination can result in a boosting phenomenon that is misdiagnosed as a TST conversion. The occurrence of boosting phenomena has been documented in 3% to 10% of Canadian HCWs Footnote 13Footnote 51. Therefore, a two-step TST is recommended (refer to Chapter 4, Diagnosis of Latent Tuberculosis Infection). PHAC has developed a compendium of the expected prevalence of TST positivity in various Canadian populations; refer to Chapter 12, Contact Follow-up and Outbreak Management in Tuberculosis Control, for a summary table from the compendium.
Periodic TST (specific clinical personnel in hospitals not considered low risk or those performing high-risk activities in all health care settings)
Recommendations for serial screening of specific HCWs for LTBI are given in the box below. Periodic TSTs should not be performed on previously TST-positive HCWs as there is no value in doing so; rather, they should be referred for medical evaluation by a physician experienced in TST interpretation and treatment of LTBI, and should also be educated on the signs and symptoms of active TB disease (refer to Chapter 3, Diagnosis of Active Tuberculosis and Drug Resistance). Information on performing a TST, the definition of skin test conversion and management of the TST-positive worker can be found in Chapter 4. Diagnosis of Latent Tuberculosis Infection.
Post-exposure TST (all hospitals)
Any HCW who has unprotected exposure (termed an exposure episode) to a patient eventually confirmed to have respiratory TB disease should be considered at risk of having been infected. This includes situations in which a patient with undiagnosed respiratory TB disease was not in an AIIR or was cared for by a HCW who was not wearing a respirator. Exposure could also occur when such patients are not treated for a sufficient amount of time or with an effective regimen before isolation is discontinued.
Recommendations for screening HCWs for LTBI
(Strong recommendations, based on moderate evidence)
- Baseline two-step TST for all HCWs upon starting work. An exception applies where documented results of a prior two-step TST exist, in which case a single-step TST should be given and prior TST results transcribed into the HCW's health record.
- Annual TST for HCWs (with negative baseline TSTs ) involved in intermediate-risk activities in health care settings not considered low risk and those involved in high-risk activities in all health care settings (refer to Tables 2 and 3).
Note: After 2 or more years of annual screening, if the annual risk of infection (based on TST conversion rate in those screened) is shown to be less than 0.5%, consideration could be given to reducing the frequency of screening to every other year or to developing criteria that restrict annual screening to fewer workers who are at higher risk, and not testing the remaining workers except after exposure.
Recommendations for screening HCWs for LTBI
(Strong recommendations, based on moderate evidence)
Post-exposure:
- Single TST 8 weeks after exposure for TST-negative HCWs exposed to people with respiratory TB disease without adequate protection.
- For previously TST-positive HCWs exposed to people with respiratory TB disease without adequate protection:
- Refer for medical evaluation and educate on signs and symptoms of active TB disease. Refer Chapter 3, Diagnosis of Active Tuberculosis and Drug Resistance.
- For HCWs with a history of BCG vaccination, refer Chapter 4, Diagnosis of Latent Tuberculosis Infection, for information on the use of interferon-gamma release assays.
Protocols for TST can be found in Chapter 4, Diagnosis of Latent Tuberculosis Infection.
Any HCW who has unprotected exposure (termed an exposure episode) to a patient eventually confirmed to have respiratory TB disease should be considered at risk of having been infected. This includes situations in which a patient with undiagnosed respiratory TB disease was not in an AIIR or was cared for by a HCW who was not wearing a respirator. Exposure could also occur when such patients are not treated for a sufficient amount of time or with an effective regimen before isolation is discontinued.
Interferon-gamma release assay (IGRA)
The use of IGRA for serial (repeated) testing of HCWs is not recommended because serial testing studies have shown high rates of conversions and reversions, unrelated to exposure or treatment. There is no consensus on the appropriate cut-offs for deciding on IGRA conversions and reversions, and data show substantial variability in IGRA results around the cut-off used for LTBI diagnosis. Thus, TST is the preferred test for serial testing for new LTBI (refer to Chapter 4, Diagnosis of Latent Tuberculosis Infection, for details).
IGRAs may be useful for confirming a positive TST in low-risk HCWs who are found positive on baseline TST as part of their pre-employment screening.
BCG vaccination
The efficacy of BCG vaccination against M. tuberculosis has varied from zero to more than 80% in randomized controlled trials Footnote 52. As a result, it is not recommended that HCWs be routinely vaccinated with BCG. Refer to Chapter 16, Bacille Calmette-Guérin (BCG) Vaccination in Canada, for details about the vaccine. The issue more relevant to most health care settings in Canada is how to interpret a positive TST or IGRA when there is a history of BCG vaccination in adulthood (refer to Chapter 4, Diagnosis of Latent Tuberculosis Infection, for information on this). Also, refer to The Online TST/IGRA interpreter![]() . A summary of the provincial and territorial usage of BCG over time is available from PHAC at the Tuberculosis Prevention and Control
. A summary of the provincial and territorial usage of BCG over time is available from PHAC at the Tuberculosis Prevention and Control![]() website and a BCG world atlas is available at BCG World Atlas: A Database of Global BCJ Vaccination Policies and Practices
website and a BCG world atlas is available at BCG World Atlas: A Database of Global BCJ Vaccination Policies and Practices![]() .
.
Adherence to TB Infection Prevention and Control Measures
Low adherence to TB infection prevention and control measures by HCWs and to treatment of LTBI by both HCWs and patients will impede TB prevention efforts. Pre-employment screening for active TB disease is not sufficient to prevent M. tuberculosis transmission incidents involving HCWs in health care settings. Periodic HCW screening, recommended as above, and a high index of suspicion coupled with early assessment of HCWs with symptoms suggestive of TB are needed. Employers have reported greater success in encouraging HCWs to participate in screening programs when they are performed in conjunction with some other required activity (e.g. orientation, WHMIS [Workplace Hazardous Materials Information System] training, employee updates, vaccination days) Footnote 14. Administrative controls such as HCW training and education, in addition to a convenient schedule and location for screening, can increase adherence to TB infection prevention and control measures Footnote 7Footnote 53.
Infection Prevention and Control of M. Tuberculosis in Specific Units and Populations Within Hospitals
Specific Units
All patients exhibiting signs and symptoms of TB in a hospital setting should be assessed to rule out active TB disease. In certain units, special consideration is required to prevent the transmission of TB to HCWs, other patients and visitors. A unit that treats or cares for at-risk patients (e.g. chemotherapy, HIV and dialysis units) should have a plan in place for how it will manage a patient with respiratory TB disease so that the patient's treatment is not interrupted and other people are not exposed.
Recommendations for Screening HCWs for LTBI
(Strong recommendations, based on strong evidence)
- Intensive care unit (ICU): Every patient with suspected or confirmed respiratory TB disease who requires care in an ICU should be placed in an appropriately ventilated AIIR within the ICU. If this is not available, arrangements should be made to transfer the patient to a facility with an AIIR within the ICU as quickly as possible. For patients requiring intubation and mechanical ventilation, an appropriate bacterial filter should be placed on the endotracheal tube to prevent contamination of the ventilator and the ambient air Footnote 16. When endotracheal suctioning is performed a closed suction apparatus should be used.
- Emergency department: A high index of suspicion for TB is required when assessing patients presenting with signs and symptoms of respiratory TB disease. Such patients should be immediately transferred to an AIIR. If such a room does not exist within the emergency department but exists elsewhere in the hospital, patients should be promptly transferred to this room until respiratory TB disease has been excluded (refer to section "Transport of patients with suspected or confirmed active respiratory TB").
- Surgery: Surgery should either be postponed (if feasible) until the TB patient is no longer considered infectious or scheduled to allow adequate ventilation of the room after surgery (refer to Table 3). Surgery is sometimes required in patients with multidrug-resistant or extensively drug resistant TB, or to drain tuberculous abscesses. Because of the presence of infectious mycobacteria (and anaesthesia gases), the air supplied to the operating room should be exhausted to the outside and not exit the room to other patient care areas. HCWs should wear appropriate respirators (refer to section "Respirators and masks"). Post-operative recovery of the patient with suspected or confirmed respiratory TB disease should take place in the operating room or in an AIIR.
Special Populations
There are certain individuals whose immunocompromising conditions or immunosuppressive therapy places them at higher risk of progression from LTBI to active TB disease Footnote 7Footnote 54. They include HIV-infected individuals, transplant patients, people undergoing anti-tumour necrosis factor therapy and those undergoing dialysis or treatment for renal disease. A high incidence of LTBI and anergy has been reported among patients with chronic renal failure requiring dialysis Footnote 55Footnote 56. The risk of active TB disease in this population appears to be high in the first 6 to 12 months after dialysis is initiated Footnote 56. Providing care for patients in a specialized clinic or in other settings might require special considerations, a higher index of suspicion for respiratory TB disease or increased vigilance to prevent transmission before diagnosis. Refer to Chapters 10 and 13 for further information. The CDC provides guidance on infection prevention and control considerations for dialysis units Footnote 7.
Prevention of Transmission of M. Tuberculosis Within Other Health Care Settings
Although the principles of TB infection prevention and control are the same across the continuum of health care, there is variation in the risk associated with different settings, and thus modification of the control measures applied is required. The availability of control measures needs to be considered when recommending interventions to prevent transmission of TB in non-hospital health care settings.
Long-term Care Facilities
Long-term care (LTC) facilities include homes for the aged, nursing homes, chronic care facilities, hospices, retirement homes, designated assisted living centres and any other collective living centre. Residents of LTC facilities are considered to be at the same risk as other populations in the community, with the exception of those belonging to at-risk groups (Refer to "Identification of patients with active respiratory TB within hospitals"). Due to the decreasing utility of TST to diagnose LTBI after age 65 and the increasing risk of adverse effects from LTBI treatment in this age group, screening with a posterior-anterior and lateral chest x-ray for active TB is preferred upon admission for those over 65 years old. Refer to Chapter 12, Contact Follow-up and Outbreak Management in Tuberculosis Control, for further discussion and references. A baseline 2-step TST is still recommended upon admission for those 65 years old and under who also belong to an identified at-risk group. Detailed screening recommendations for both HCWs and residents in LTC facilities are provided in Table 4.
Ambulatory Care/Outpatient Clinics
Ambulatory care settings include locations where health services are provided to patients who are not admitted to inpatient hospital units. This includes, but is not limited to, outpatient diagnostic and treatment facilities (e.g. diagnostic imaging, phlebotomy sites, pulmonary function laboratories, TB treatment facilities), community health centres or clinics, physician offices and offices of allied health professionals (e.g. physiotherapists) Footnote 7Footnote 16. If the patient mix includes members of at-risk populations, a high index of suspicion should be maintained for the presence of respiratory TB disease. Refer to section "Identification of patients with active respiratory TB within hospitals" for a description of this population.
Recommendations
(Conditional recommendations, based on weak evidence)
-
If possible, visits by people with suspected or confirmed respiratory TB disease should be postponed until no longer infectious.
- If a visit cannot be postponed, it should be scheduled at the end of the day to minimize exposure to others, and, when possible, staff should be alerted of these visits to allow for prompt use of precautions Footnote 16.
- The patient should be provided with a mask before arrival or immediately upon reception to be worn until an AIIR becomes available. If unavailable, the patient should be temporarily assessed or treated in a single room with the door closed, away from vulnerable patients, and transferred as soon as medically feasible to a facility with AIIRs if admission is required Footnote 16.
- HCWs caring for people with suspected or confirmed respiratory TB disease in outpatient clinics should wear a respirator (Refer to section "Respirators and masks").
- Refer to Table 4 for further infection prevention and control recommendations for this setting.
Paramedics and Other Emergency Medical Services
Exposure to airborne infectious agents remains a substantial hazard for emergency medical services (EMS) providers. Such exposure can occur during resuscitation or routine transportation of patients.
Recommendation
(Strong recommendation, based on strong evidence)
EMS providers should wear appropriate respirators when attending to people with suspected or confirmed respiratory TB disease. Refer to section "Transport of patients with suspected or confirmed active respiratory TB."
Remote and Isolated Health Care Settings
In remote and isolated communities there are many challenges to TB infection prevention and control. Resource limitations may result in difficulties with access to adequate diagnostic facilities for bacteriologic examinations and chest radiography. In some remote and isolated First Nations and Inuit communities, the average TB incidence rates are high but vary considerably among communities Footnote 57. Refer to Chapter 14, Tuberculosis Prevention and Care in First Nations, Inuit and Métis Peoples.
Respiratory TB disease should be ruled out for anyone presenting with unexplained cough for more than 2 weeks with or without fever, unexplained weight loss, hemoptysis, loss of appetite and night sweats. This requires a chest radiograph and analysis of three sputum smears for AFB. The most important measure for infection prevention and control is a high index of suspicion in members of at-risk populations (refer to section "Identification of patients with active respiratory TB within hospitals") with rapid use of diagnostic procedures (including sputum examinations and chest radiography) and early initiation of therapy. If chest radiography is difficult to organize because patients must fly out of the community, then sending sputum samples for AFB smear and TB culture may be a more rapid way to make a diagnosis.
Recommendations
(Strong recommendations, based on moderate evidence)
- In high-prevalence areas where primary care nurses may be required to collect sputum samples for examination for AFB, they should wear a respirator and separate themselves from the area where the person is providing the sputum specimen.
- Health care facilities that care for at-risk populations should have access to resources that will facilitate implementation of essential administrative, environmental and personal protective controls.
- Refer to Table 4 for further infection prevention and control recommendations for this setting.
Where resources remain limited because of lack of the infrastructure needed to implement necessary infection prevention and control measures, strategies used in low-resource countries could be implemented: Footnote 58
- Schedule visits from people with suspected or confirmed respiratory TB disease at the end of the day or after regular hours.
- If patients needing medical attention cannot be transferred to a facility with an AIIR, cohort smear- positive TB patients, provided they are receiving treatment and there is no suspicion of drug resistance (or the prevalence of drug-resistance is known to be very low) Footnote 26.
- Establish effective out-patient services with community-based treatment programs (in homes) to complete treatment started in the hospital, especially where AIIRs are unavailable Footnote 58.
- When outdoor temperature permits, use natural ventilation to assist in reducing the risk of transmission of airborne pathogens. The World Health Organization has produced evidence-based guidelines on natural ventilation with minimal hourly ventilation rates Footnote 59.
Home Care Settings
Home care is delivered to patients who reside in their home or a community care residence. M. tuberculosis transmission to HCWs who work in home-based health care settings has been documented with recommendations developed to prevent transmission Footnote 7. The room in the home where the patient spends considerable amounts of time should be well ventilated Footnote 16.
Recommendations
(Conditional recommendations, based on very weak evidence)
- Home care agencies in consultation with public health authorities should develop a system for screening at-risk clients for signs of respiratory TB disease before and during visits, thus facilitating earlier diagnosis and use of appropriate infection prevention and control measures.
- HCWs caring for clients with respiratory TB disease at home should wear a respirator (refer to section "Respirators and masks").
- HCWs should not perform cough-inducing or aerosol-generating medical procedures on clients with suspected or confirmed infectious TB disease, because recommended infection prevention and control measures will probably not be in place in the home Footnote 7.
- Refer to Table 4 for further infection prevention and control recommendations for this setting.
- Refer to Figure 2 on home isolation and Chapter 5, Treatment of Tuberculosis Disease.
Prevention of Transmission of M. Tuberculosis Within Residential and Community Care Settings
While guidance is available on preventing M. tuberculosis transmission in health care settings, less has been written about prevention in community care settings, even though the incidence of LTBI and active TB disease in these settings exceeds that in the general population who are not receiving care Footnote 60.
Adult Day Care Centres
For the purposes of these guidelines, adult day care facilities include basic or specialized day care centres for adults or other special adult populations requiring care. Adult day care services often include group programs designed to meet the social and health needs of functionally and/or cognitively impaired adults. Examples of clients include individuals with Alzheimer's disease, developmental disabilities, traumatic brain injury, mental illness, vision and hearing impairments Footnote 37. Refer to Table 4 for screening recommendations for clients and employees. These recommendations apply only to clients who expect to use these services for 4 or more hours per week or for 150 or more hours per year.
Homeless Shelters and Drop-in Centres
Recent extended outbreaks of M. tuberculosis in homeless and under-housed individuals in Canada and the United States highlight the risk of ongoing transmission within this population Footnote 61Footnote 62. Overcrowding increases transmission risk, as does failure to recognize signs and symptoms of respiratory TB disease and inability to take immediate steps to prevent transmission. An upsurge in foreign-born homeless people in Canada could present an increased risk of drug-resistant strains being introduced into the homeless shelter system Footnote 6. Employees and regular volunteers of shelters are at increased risk of becoming infected with TB because of frequent exposure to undiagnosed cases, compounded by inadequate ventilation. Screening for LTBI among the homeless can be labour intensive and complicated, and adherence to therapy for LTBI is often low in this population. Active case finding can also be challenging, as a large proportion of homeless people may have chronic cough and other symptoms that can imitate those of TB. Furthermore, following up on contacts of active cases can be extremely difficult.
Primary prevention of TB through improved environmental controls is perhaps the most important control strategy. This includes cleaning, repair and upgrading of air filter units as well as adding in-duct and upper-air UVGI, which will help reduce the risk of TB transmission Footnote 63. Opening windows to improve fresh air ventilation can also result in a dramatic decrease in M. tuberculosis transmission, especially in shelters with inadequate ventilation Footnote 64. However, this is not feasible for most of the year in Canada because of cold temperatures. Guidelines to assist shelter operators and staff in reducing the risk of M. tuberculosis transmission in homeless shelters have been published Footnote 64Footnote 65.
Recommendations
(Conditional recommendations, based on very weak evidence)
- With support from local public health authorities, homeless shelters should develop and implement a TB management program that provides education to staff, volunteers and clients.
- Refer to Table 4 for further infection prevention and control recommendations for this setting.
Addiction Treatment Centres
A high prevalence of positive TST concurrent with increasing duration of injection drug use has been documented in this population. In addition, drug users have also been shown to have an increased risk of progression from LTBI to active TB disease Footnote 10. The benefit of TST screening for this high-risk population in terms of follow-up medical evaluation and adherence to therapy has been low Footnote 10. Incentives have been shown to be a consistent and effective strategy for increasing participation in TB screening as well as educational activities for this population Footnote 10Footnote 66. Refer to Table 4 for further recommendations for this setting.
In populations known to have poor rates of return for TST reading (e.g. homeless individuals and intravenous drug users), use of IGRAs can help achieve a higher rate of test completion and follow-up, although completion of LTBI treatment may still be challenging.
Prevention of Transmission of M. Tuberculosis Within Correctional Facilities
The following is based in part on the Correctional Service Canada (CSC) guidelines for TB prevention and control in institutions in which inmates are sentenced to 2 years or longer Footnote 67. At the time of publication of this Standard, the CSC guidelines were under revision. An additional resource is the guideline published by the CDC on the prevention and control of TB in US correctional and detention facilities Footnote 68. It should be noted that the recommendations below were developed mainly for federal facilities, as TB prevention and control activities and capacity vary across Canada for provincial/territorial correctional facilities. The latter facilities generally have more inmates, most of whom have shorter stays than inmates in federal facilities. The shorter duration of incarceration in provincial/territorial facilities, make it more difficult to implement recommendations developed for federal facilities.
The risk of TB transmission is higher in correctional facilities as a result of several factors:
- The prevalence of LTBI among correctional facility inmates is higher than in the average Canadian population.
- The risk of reactivation of LTBI to active TB disease is increased because of the higher prevalence of HIV infection, other comorbidities, previous or current cigarette smoking, and alcohol and injection drug abuse in this population.
- Diagnosis may be delayed because of poor use of medical services.
- Ventilation is often inadequate because of recirculation of air and a lack of open windows. This is more common in older prisons that were built to achieve security, not airborne infection control.
- The density of inmates may be high (crowding).
- Transfer of inmates within and between facilities may be frequent.
TB Control Program for Correctional Facilities
It is recommended that the first step of a TB management program in a correctional facility should be to perform an institutional risk assessment in order to decrease the risk of inmate and staff exposure to and acquisition of M. tuberculosis. This risk assessment is based on the baseline TB status of inmates and staff and an annual review of active respiratory TB cases diagnosed among inmates (and, if any, among staff). This involves inquiries into the medical and TB history as well as risk factors and symptoms. Past TB-related history should be collected, if necessary, by accessing a comprehensive electronic medical database. The history should be reviewed carefully, including results of previous TSTs and any chest radiography, as should prior treatment of LTBI or active TB disease. Incomplete treatment should prompt a thorough evaluation of the possibility of active TB disease by means of chest radiography, medical evaluation and sputum analysis for AFB smears and cultures. Active case finding by symptom check is recommended for inmates on admission (baseline) and annually thereafter. At all other times a high index of suspicion should be maintained in order to minimize delays in the diagnosis of active respiratory TB. Suspicion should be particularly high if the inmate has a prior history of TB, even if treatment was judged to have been adequate, since actual adherence to treatment may have been suboptimal, leading to increased risk of relapse.
AIIRs exist across Canada in CSC facilities with at least one per geographic/administrative region. The direction of air flow should be into the room, and the air should then be exhausted outdoors. This should be verified when the room is occupied. For treatment of LTBI in inmates and staff, refer to Chapter 6, Treatment of Latent Tuberculosis Infection.
Recommendations
(Strong recommendations, based on strong evidence)
- Inmates who are suspected of having respiratory TB disease should be placed immediately in an AIIR until TB is ruled out or they have received sufficient treatment and are deemed no longer infectious (Refer to Figure 1).
- Inmates and staff who are exposed to people with respiratory TB disease should be investigated in close collaboration with local public health authorities using the principles outlined in Chapter 12, Contact Follow-up and Outbreak Management in Tuberculosis Control.
- Refer to Table 4 for further infection prevention and control recommendations for this setting.
- If an inmate is discharged while still being treated for active TB disease, follow-up should be arranged directly with local public health authorities, so that supervised treatment is not interrupted, even for a day.
| Facility/setting | Administrative controls | Environmental controls Table 4 - Footnote A | Personal respiratory protection controls | Screening and surveillance Table 4 - Footnote B |
|---|---|---|---|---|
| Table 4. Legend
| ||||
| Long-term care (homes for the aged, nursing homes, chronic care facilities, hospices, retirement homes, designated assisted living centres and any other collective living centre) | Facility risk assessment by retrospective review of all TB cases in preceding 5 years and all available TST results for staff and volunteers. This should inform the decision to routinely screen residents. Educate staff about TB symptoms, risk factors and infection prevention and control measures Table 4 - Footnote C. People with infectious TB should be transported as soon as possible to an appropriate medical facility and should not return to the setting until they are no longer infectious. | CTS: 2 ACH CSA: 4 ACH CDC : NR FGI/ASHRAE: 2-6 ACH | Respirators for HCWs in contact with people with infectious TB Table 4 - Footnote D. Mask for people with infectious TB if not in airborne infection isolation room (AIIR) and during transport. | Employees/volunteers Table 4 - Footnote E: Baseline screening upon hire or placement using two-step TST Table 4 - Footnote F. Annual TST unless conversion rate is shown to be ≤0.5% Table 4 - Footnote G. |
| Residents/clients: Baseline posterior-anterior and lateral chest radiography on admission for people >65 years old from identified populations Table 4 - Footnote H. Baseline two-step TST upon admission for identified population £65 years old Table 4 - Footnote F. Annual TST not necessary. Facility risk assessment/local epidemiology should inform decision Table 4 - Footnote I. | ||||
| Ambulatory care and outpatient clinics Refer to Table 2 for ACH recommendations for AIIR | Signage at entry requesting use of surgical mask by people with respiratory symptoms that suggest infection. High index of suspicion if signs and symptoms of active TB disease. Schedule visit by people with infectious TB for end of day. | CTS: 2 ACH CSA: 6-9 ACH CDC : NR FGI/ASHRAE: 6 ACH | Respirators for HCW in contact with people with infectious TB Table 4 - Footnote D. Mask for people with infectious TB if not in AIIR or during transport. | Employees/volunteers Table 4 - Footnote E: Baseline screening upon hire or placement using two-step TST Table 4 - Footnote F. Annual TST not necessary. |
| Patients: Refer to Chapter 13, Tuberculosis Surveillance and Screening in High-risk Populations, for information on which individuals should be screened. | ||||
| Clinic or nursing station etc. in remote and isolated settings or communities Refer to Table 2 for ACH recommendations for AIIR | Schedule visits for people with infectious TB at the end of the day or after hours. Educate staff on TB symptoms, risk factors and infection control measures. Community-based treatment program (refer Figure 2 on home isolation). Patient with infectious TB who cannot be medically managed at home should be transferred to an appropriate hospital as soon as possible. | CTS: 2 ACH and/or UVGI to supplement CSA: 6-9 ACH CDC : NR FGI/ASHRAE: 6 ACH Natural ventilation where no mechanical ventilation exists and weather permits. | Respirators for HCWs in contact with people with infectious TB Table 4 - Footnote D. Mask for people with infectious TB if outside the home. | Employees/volunteers Table 4 - Footnote E: Baseline screening upon hire or placement using two-step TST Table 4 - Footnote F. Annual TST if previously negative and people with infectious TB are being seen in the facility. Otherwise, annual TST is not necessary Table 4 - Footnote G. |
| Patients: Refer to Chapter 13, Tuberculosis Surveillance and Screening in High-Risk Populations, regarding which individuals should be screened upon admission. | ||||
| Home care | Educate staff on TB symptoms, risk factors and infection prevention and control measures. Refer to Figure 2 for home isolation recommendation. | ACH: NA People with infectious TB should not share common airspace with non-household members. Use of natural ventilation when weather permits. | Respirators for HCWs in contact with people with infectious TB Table 4 - Footnote D. Mask for people with infectious TB if leaving home for necessary appointment. | Employees/volunteers Table 4 - Footnote E: Baseline screening upon hire or placement using two-step TST Table 4 - Footnote F. Annual TST if employee's results were previously negative and agency provides care for people with infectious TB. Otherwise, annual TST is not necessary Table 4 - Footnote G. |
| Clients: NA | ||||
| Adult day care centres | Refer to recommendations for long-term care (LTC) above. | NR | Refer LTC above. | Refer to recommendations for LTC above. |
| Homeless shelters Drop-in centres Addiction treatment centres | TB management program. Educate staff on TB symptoms, risk factors and infection prevention and control measures. Head-to-foot bed arrangement. Incentives and enablers may be considered to encourage resident screening for LTBI. People with infectious TB should be immediately placed in a separate room, transported to an appropriate health care facility and returned only when they are no longer infectious. | CTS: 6 or 0.708 m3/min/person Table 4 - Footnote J. CSA: NR CDC : 25 cubic feet of outside air/minute/person FGI/ASHRAE: NR Maintenance and upgrade of HVAC filter units as required. UVGI Table 4 - Footnote L Use of natural ventilation where no mechanical ventilation exists and weather permits. | Respirators for HCWs performing medical assessment of people with infectious TB prior to transfer for medical care Table 4 - Footnote D. Mask for people with infectious TB pending and during transport to a health care facility. | Employees/volunteers Table 4 - Footnote E: Baseline screening upon hire or placement using two-step TST Table 4 - Footnote F. Annual TST if negative Table 4 - Footnote G. |
| Clients: Refer to Chapter 13, Tuberculosis Surveillance and Screening in High-risk Populations, for information on which individuals should be screened. In outbreaks consider outbreak case finding. | ||||
| Correctional facilities | Airborne precautions (refer to Figure 1 legend) for people with infectious TB until deemed no longer infectious. Supervised therapy for people with infectious TB. Educate inmates on importance of completing therapy and on precautions. High index of suspicion for active respiratory TB. If possible, separate housing of symptomatic new inmates until screened for respiratory TB disease. Health teaching for people with respiratory TB disease to increase isolation and treatment adherence. | General inmates areas: CTS: 2 ACH CSA: NR CDC : 6-12 ACH FGI/ASHRAE: NR AIIR : HEPA filtration Table 4 - Footnote K. | Respirators for HCWs and prison staff in contact with people with infectious TB Table 4 - Footnote D. Mask for people with infectious TB if not in AIIR or during transport. | Employees/volunteers: Baseline screening upon hire or placement using two-step TST Table 4 - Footnote F. Baseline assessment for signs, symptoms and risk factors for TB. Annual TST if negative Table 4 - Footnote G. Annual assessment for signs and symptoms of active TB disease. |
| Inmates: If >1 year stay, baseline screening at admission using two-step TST Table 4 - Footnote F. Returning inmates receive a single-step TST. Annual TST thereafter (if TST negative) and assessment of risk factors for active TB disease Table 4 - Footnote G. Annual assessment of signs and symptoms for inmates with positive TST or history of TB, and medical examination for inmates with symptoms of active TB disease. If <1 year stay, assess for symptoms and signs of TB, past history of TB and known immunosuppression at admission. If any of these is present, chest radiography and medical evaluation should be done. | ||||
References
- Footnote 1
- Menzies D, Fanning A, Yuan L, et al. Hospital ventilation and risk for tuberculous infection in Canadian health care workers. Ann Intern Med 2000;133:779-89. http://annals.org/article.aspx?articleid=714002.
- Footnote 2
- Menzies D, Fanning A, Yuan L, et al. Factors associated with tuberculin conversion in Canadian microbiology and pathology workers. Am J Respir Crit Care Med 2003;167:599-602. http://www.atsjournals.org/doi/abs/10.1164/rccm.200208-873BC?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed.
- Footnote 3
- Menzies D, Lewis M, Oxlade O. Costs for tuberculosis care in Canada. Can J Public Health 2008;99:391-6. http://www.ncbi.nlm.nih.gov/pubmed/19009923.
- Footnote 4
- Menzies D, Fanning A, Yuan L, et al. Tuberculosis among health care workers. New Engl J Med 1995;332:92-8. http://www.nejm.org/doi/full/10.1056/NEJM199501123320206.
- Footnote 5
- Menzies D, Joshi R, Pai M. Risk of tuberculosis infection and disease associated with work in health care settings. Int J Tuberc Lung Dis 2007;11:593-605. http://www.ncbi.nlm.nih.gov/pubmed/17519089.
- Footnote 6
- Khan K, Rea E, McDermaid C, et al. Active tuberculosis among homeless persons, Toronto, Ontario, Canada, 1998-2007. Emerg Infect Dis 2011;17:357-65. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3166000/pdf/10-0833_finalR.pdf.
- Footnote 7
- Centers for Disease Control and Prevention. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings. MMWR 2005;54:1-142. http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5417a1.htm.
- Footnote 8
- Greenaway C, Sandoe A, Vissandjee B, et al. Tuberculosis: evidence review for newly arriving immigrants and refugees. Can Med Assoc J 2011;183:E939-E951. http://www.cmaj.ca/content/183/12/E939.long.
- Footnote 9
- Baussano I, Nunn P, Williams B, et al. Tuberculosis among health care workers. Emerg Infect Dis 2011;17:488-94. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3298382/.
- Footnote 10
- Brassard P, Bruneau J, Schwartzman K, et al. Yield of tuberculin screening among injection drug users. Int J Tuberc Lung Dis 2004;8:988-93. http://www.ncbi.nlm.nih.gov/pubmed/15305482.
- Footnote 11
- Trajman A, Menzies D. Occupational respiratory infections. Curr Opin Pulm Med 2010;16:226-34. http://www.ncbi.nlm.nih.gov/pubmed/20375784.
- Footnote 12
- Catanzaro A. Nosocomial tuberculosis. Am Rev Respir Dis 1982;125:559-62. http://www.ncbi.nlm.nih.gov/pubmed/7081816.
- Footnote 13
- Menzies D, Fanning A, Yuan L, et al. Tuberculosis in health care workers: a multicentre Canadian prevalence survey: preliminary results. Int J Tuberc Lung Dis 1998;2:S98-S102. http://www.ncbi.nlm.nih.gov/pubmed/9755973.
- Footnote 14
- Public Health Agency of Canada (formerly Health Canada). Guidelines for preventing the transmission of tuberculosis in Canadian health care facilities and other institutional settings. CCDR 1996;22S1. http://www.collectionscanada.gc.ca/webarchives/20071120001332/http:/www.phac-aspc.gc.ca/publicat/ccdr-rmtc/96vol22/22s1/index.html.
- Footnote 15
- Public Health Agency of Canada, Canadian Lung Association. Canadian Tuberculosis Standards. 6th ed. Ottawa, Ont., 2007. https://www.lung.ca/cts-sct/pdf/tbstand07_e.pdf.
- Footnote 16
- Public Health Agency of Canada. Routine practices and additional precautions for preventing the transmission of infection in healthcare settings. Ottawa, ON: PHAC, 2013. http://www.phac-aspc.gc.ca/nois-sinp/guide/pubs-eng.php.
- Footnote 17
- Sterling TR, Zhao Z, Khan A, et al. Mortality in a large tuberculosis treatment trial: modifiable and non-modifiable risk factors. Int J Tuberc Lung Dis 2006;10:542-9. http://www.ncbi.nlm.nih.gov/pubmed/16704037.
- Footnote 18
- Conde MB, Loivos AC, Rezende VM, et al. Yield of sputum induction in the diagnosis of pleural tuberculosis. Am J Respir Crit Care Med 2003;167:723-5. http://www.ncbi.nlm.nih.gov/pubmed/12598215.
- Footnote 19
- Greenaway C, Menzies D, Fanning A, et al. Delay in diagnosis among hospitalized patients with active tuberculosis - predictors and outcomes. Am J Respir Crit Care Med 2002;165:927-33. http://www.atsjournals.org/doi/abs/10.1164/ajrccm.165.7.2107040?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed.
- Footnote 20
- Crofts JP, Andrews NJ, Barker RD, et al. Risk factors for recurrent tuberculosis in England and Wales, 1998-2005. Thorax 2010;65:310-4. http://thorax.bmj.com/content/65/4/310.long.
- Footnote 21
- Muecke C, Isler M, Menzies D, et al. The use of environmental factors as adjuncts to traditional tuberculosis contact investigation. Int J Tuberc Lung Dis 2006;10:530-5. http://www.ncbi.nlm.nih.gov/pubmed/16704035.
- Footnote 22
- Beggs CB, Noakes CJ, Sleigh PA, et al. The transmission of tuberculosis in confined spaces: an analytical review of alternative epidemiological models. Int J Tuberc Lung Dis 2003;7:1015-26. http://www.ncbi.nlm.nih.gov/pubmed/14598959.
- Footnote 23
- Great Britain Medical Research Council. BCG and vole bacillus vaccines in the prevention of tuberculosis in adolescence and early life. Brit Med J 1963;1:973-8. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2480749/.
- Footnote 24
- World Health Organization. Tuberculosis prevention, care and control - a practical directory of new advances. Geneva: WHO, Report No. WHO/HTM/TB/2011.20, 2011. http://whqlibdoc.who.int/publications/2011/9789241502658_eng.pdf.
- Footnote 25
- World Health Organization. Global tuberculosis control. Geneva: WHO, Report No. WHO/HTM/TB/2011.16, 2011. http://www.who.int/tb/publications/global_report/2011/en/.
- Footnote 26
- World Health Organization. WHO policy on TB infection control in health-care facilities, congregate settings and households. Geneva: WHO, Report No. WHO/HTM/TB/2009.419. http://www.ncbi.nlm.nih.gov/books/NBK179249/.
- Footnote 27
- Rao VK, Iademarco EP, Fraser VJ, et al. Delays in the suspicion and treatment of tuberculosis among hospitalized patients. Ann Intern Med 1999;130:404-11. http://annals.org/article.aspx?articleid=712593.
- Footnote 28
- Long R, Zielinski M, Kunimoto D, et al. The emergency department is a determinant point of contact of tuberculosis patients prior to diagnosis. Int J Tuberc Lung Dis 2002;6:332-9. http://www.ncbi.nlm.nih.gov/pubmed/11936743.
- Footnote 29
- Beggs CB, Shepherd SJ, Kerr KG. Potential for airborne transmission of infection in the waiting areas of healthcare premises: stochastic analysis using a Monte Carlo model. BMC Infect Dis 2010;10:247. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2939637/pdf/1471-2334-10-247.pdf.
- Footnote 30
- Cruz AT, Starke JR. A current review of infection control for childhood tuberculosis. Tuberculosis 2011;91:S11-S15. http://www.ncbi.nlm.nih.gov/pubmed/22079589.
- Footnote 31
- Munoz FM, Ong LT, Seavy D, et al. Tuberculosis among adult visitors of children with suspected tuberculosis and employees at a children's hospital. Infect Control Hosp Epidemiol 2002;23:568-72. http://www.jstor.org/stable/10.1086/501972.
- Footnote 32
- Siddiqui AH, Perl TM, Conlon M, et al. Preventing nosocomial transmission of pulmonary tuberculosis: When may isolation be discontinued for patients with suspected tuberculosis? Infect Control Hosp Epidemiol 2002;23:141-4. http://www.jstor.org/stable/10.1086/502024.
- Footnote 33
- Wilmer A, Bryce E, Grant J. The role of the third acid-fast bacillus smear in tuberculosis screening for infection control purposes: a controversial topic revisited. Can J Infect Dis Med Microbiol 2011;22:e1-e3. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3076153/pdf/idmm22e001.pdf.
- Footnote 34
- Menzies D. Effect of treatment on contagiousness of patients with active pulmonary tuberculosis. Infect Control Hosp Epidemiol 1997;18:582-6. http://www.ncbi.nlm.nih.gov/pubmed/?term=Effect+of+treatment+on+contagiousness+of+patients+with+active
+pulmonary+tuberculosis.+Infect+Control+Hosp+Epidemiol. - Footnote 35
- Nardell EA, Keegan J, Cheney SA, et al. Airborne infection: theoretical limits of protection achievable by building ventilation. Am Rev Respir Dis 1991;144:302-6. http://www.ncbi.nlm.nih.gov/pubmed/1907115.
- Footnote 36
- Canadian Standards Association. Special requirements for heating, ventilation, and air-conditioning (HVAC) systems in health care facilities. Toronto, Ont.: CSA, Report No. Z317.2-10, 2010. http://books.google.ca/books?id=9VJhcgAACAAJ&dq=Special+requirements+for+heating,+ventilation,+and+air-conditioning+(HVAC)+systems+in+health+care+facilities.&hl=en&sa=X&ei=gM7oU6ivCcm2yASbyoDoCQ&ved=0CC8Q6AEwAg.
- Footnote 37
- Facility Guidelines Institute, US Department of Health and Human Services. Guidelines for design and construction of health care facilities. 2010. http://www.ashe.org/resources/publications/guidelines2010.html.
- Footnote 38
- Knibbs LD, Morawska L, Bell SC, et al. Room ventilation and the risk of airborne infection transmission in 3 health care settings within a large teaching hospital. Am J Infect Control 2011;39:866-72. http://www.sciencedirect.com/science/article/pii/S0196655311001799.
- Footnote 39
- Nardell EA. Fans, filters or rays? Pros and cons of the current environmental tuberculosis control technologies. Infect Control Hosp Epidemiol 1993;14:681-5. http://www.ncbi.nlm.nih.gov/pubmed/8132991.
- Footnote 40
- Centers for Disease Control and Prevention. Environmental control for tuberculosis: basic upper-room ultraviolet germicidal irradiation guidelines for healthcare settings. Report No. DHHS (NIOSH) Publication No. 2009-105, 2009. http://stacks.cdc.gov/view/cdc/5306.
- Footnote 41
- Reed NG. The history of ultraviolet germicidal irradiation for air disinfection. Public Health Rep 2010;125:15-27. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2789813/pdf/phr125000015.pdf.
- Footnote 42
- Coffey CC, Lawrence RB, Campbell DL, et al. Fitting characteristics of eighteen N95 filtering-facepiece respirators. J Occup Environ Hyg 2004;1:262-71. http://www.tandfonline.com/doi/abs/10.1080/15459620490433799?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed.
- Footnote 43
- Campbell DL, Coffey CC, Lenhart SW. Respiratory protection as a function of respirator fitting characteristics and fit-test accuracy. Am Ind Hyg Assoc J 2001;62:36-44. http://www.ncbi.nlm.nih.gov/pubmed/11258866.
- Footnote 44
- Centers for Disease Control and Prevention. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care facilities. MMWR 1994;43:1-132. http://www.cdc.gov/mmwr/preview/mmwrhtml/00035909.htm.
- Footnote 45
- Dharmadhikari AS, Mphalele M, Stoltz A, et al. Surgical face masks worn by patients with multidrug-resistant tuberculosis - impact on infectivity of air on a hospital ward. Am J Respir Crit Care Med 2012;185:1104-9. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3359891/.
- Footnote 46
- Fennelly KP, Nardell EA. The relative efficacy of respirators and room ventilation in preventing occupational tuberculosis. Infect Control Hosp Epidemiol 1998;19:754-9. http://www.ncbi.nlm.nih.gov/pubmed/9801283.
- Footnote 47
- Lawrence RB, Duling MG, Calvert CA, et al. Comparison of performance of three different types of respiratory protection devices. J Occup Environ Hyg 2006;3:465-74. http://www.tandfonline.com/doi/abs/10.1080/15459620600829211?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed.
- Footnote 48
- Danyluk Q, Hon CY, Neudorf M, et al. Health care workers and respiratory protection: Is the user seal check a surrogate for respirator fit-testing? J Occup Environ Hyg 2011;8:267-70. http://www.tandfonline.com/doi/abs/10.1080/15459624.2011.566016?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed.
- Footnote 49
- Centers for Disease Control and Prevention. Laboratory performance evaluation of N95 filtering facepiece respirators. MMWR 1998;47:1045-9. http://www.cdc.gov/mmwr/preview/mmwrhtml/00055954.htm.
- Footnote 50
- Canadian Standards Association. Selection, use, and care of respirators. Toronto, Ont.: Report No. Z94.4-11, 2011. https://www.google.ca/url?url=https://portal.csse.org/opendoc.asp%3FdocID%3D2496&rct=j&frm=1&q=&esrc=s&
sa=U&ei=6hXlU-fNAYeYyQTr-ILICg&ved=0CBMQFjAA&usg=AFQjCNEWYXgHMkS5qu4OrpqPlco3t17YRA. - Footnote 51
- Menzies R, Vissandjee B, Rocher I, et al. The booster effect in two-step tuberculin testing among young adults in Montreal. Ann Intern Med 1994;120:190-8. http://annals.org/article.aspx?articleid=707079.
- Footnote 52
- Colditz GA, Brewer TF, Berkey CS, et al. Efficacy of BCG vaccine in the prevention of tuberculosis: meta-analysis of the published literature. JAMA 1994;271:698-702. http://jama.jamanetwork.com/article.aspx?articleid=366365.
- Footnote 53
- Joseph HA, Shrestha-Kuwahara R, Lowry D, et al. Factors influencing healthcare workers' adherence to work site tuberculosis screening and treatment policies. Am J Infect Control 2004;32:456-61. http://www.sciencedirect.com/science/article/pii/S0196655304004791.
- Footnote 54
- Gardam MA, Keystone EC, Menzies R, et al. Anti-tumour necrosis factor agents and tuberculosis risk: mechanisms of action and clinical management. Lancet Infect Dis 2003;3:148-55. http://www.sciencedirect.com/science/article/pii/S1473309903005450.
- Footnote 55
- Smirnoff M, Patt C, Seckler B, et al. Tuberculin and anergy skin testing of patients receiving long-term hemodialysis. Chest 1998;113:25-7. http://journal.publications.chestnet.org/article.aspx?articleid=1071240.
- Footnote 56
- Chia S, Karim M, Elwood RK, et al. Risk of tuberculosis in dialysis patients: a population-based study. Int J Tuberc Lung Dis 1998;2:989-91. http://www.ncbi.nlm.nih.gov/pubmed/9869114.
- Footnote 57
- Pepperell C, Chang AH, Wobeser W, et al. Local epidemic history as a predictor of tuberculosis incidence in Saskatchewan Aboriginal communities. Int J Tuberc Lung Dis 2011;15:899-905. http://www.ncbi.nlm.nih.gov/pubmed/21682962.
- Footnote 58
- Nardell E, Dharmadhikari A. Turning off the spigot: reducing drug-resistant tuberculosis transmission in resource-limited settings. Int J Tuberc Lung Dis 2010;14:1233-43. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3709569/pdf/nihms487670.pdf.
- Footnote 59
- World Health Organization. Natural ventilation for infection control in health-care settings. Geneva: WHO, Report No. 1, 2009. http://www.who.int/water_sanitation_health/publications/natural_ventilation.pdf.
- Footnote 60
- Jarvis M. Tuberculosis: infection control in hospital and at home. Nursing Standards 2010;25:41-7. http://www.ncbi.nlm.nih.gov/pubmed/20949823.
- Footnote 61
- Adam HJ, Guthrie JL, Bolotin S, et al. Genotypic characterization of tuberculosis transmission within Toronto's under-housed population, 1997-1998. Int J Tuberc Lung Dis 2010;14:1350-3. http://www.ncbi.nlm.nih.gov/pubmed/20843430.
- Footnote 62
- Aspler A, Chong H, Kunimoto D, et al. Sustained intra- and interjurisdictional transmission of tuberculosis within a mobile, multi-ethnic social network: lessons for tuberculosis elimination. Can J Public Health 2010;101:205-9. http://www.ncbi.nlm.nih.gov/pubmed/20737810.
- Footnote 63
- Coffey CC, Hudnall JB, Martin SB. Improving the environmental controls at a homeless shelter to assist in reducing the probability of airborne transmission of Mycobacterium tuberculosis: a case study. Indoor Built Environ 2009;18:168-82. http://ibe.sagepub.com/content/18/2/168.refs.
- Footnote 64
- Francis J. Curry National Tuberculosis Center, California Department of Health Services. TB in homeless shelters: reducing the risk through ventilation, filters, and UV. 2000. http://books.google.ca/books/about/TB_in_Homeless_Shelters.html?id=JFQ0HAAACAAJ&redir_esc=y.
- Footnote 65
- Toronto Public Health. Environmental control best practices: guidelines to reduce TB transmission in homeless shelters and drop-in centres. 2007. http://www.tbonline.info/archive/document/74/.
- Footnote 66
- Marra CA, Marra F, Cox VC, et al. Factors influencing quality of life in patients with active tuberculosis. Health & Quality of Life Outcomes 2004;2:58. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC526389/.
- Footnote 67
- Correctional Service Canada, Health Canada. Tuberculosis prevention and control guidelines for federal correctional institutions (provisional). 2004.
- Footnote 68
- Centers for Disease Control and Prevention. Prevention and control of tuberculosis in correctional and detention facilities: recommendations from CDC. MMWR 2006;55:1-44. http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5509a1.htm.
- Footnote 69
- Centers for Disease Control and Prevention. Prevention and control of tuberculosis among homeless persons. Recommendations of the Advisory Council for the Elimination of Tuberculosis. MMWR 1992;41:1-9. http://www.cdc.gov/mmwr/preview/mmwrhtml/00019922.htm.
[Previous page] [Table of Contents] [Next page]
Delivering Healthcare in America 7th Edition Chapter 11
Source: https://www.canada.ca/en/public-health/services/infectious-diseases/canadian-tuberculosis-standards-7th-edition/edition-11.html